Elaine Cotter was 52 when she started to feel sudden sharp back pain after the gym. It would take her breath away. Then one day in her kitchen, she coughed. This time it was as if she’d been hit with a baseball bat. Her legs went to jelly. “I held on to the kitchen bench until my husband quickly wheeled the computer chair in so I could sit on it, and he wheeled me to the bed.”
Elaine went to hospital but doctors didn’t do an X-ray. She had a history of back pain and they believed it was to do with the arthritis she’d been diagnosed with in the past. They gave her pain medication and a walking frame. She visited several specialists over three years and received more painkillers and, eventually, antidepressants. “Everyone thought – even I thought – I just wasn’t really tolerating pain.”
One day, she was holding her new granddaughter and felt a crack in her back. ″I’m not even moving, how can I injure myself?” she thought. That’s when it clicked – maybe this was osteoporosis, a condition where the cells that maintain bone get out of balance. She had a scan along with several other X-rays that showed she had severely weakened bones in her hip and spine, including two crushed vertebrae – the hallmark of osteoporosis when bones have weakened to breaking point. “I started the journey of knowing what I had,” she says. “Not knowing was really, really bad.”
More than 1 million Australians have osteoporosis, and a further 6.3 million have low bone density. It often surfaces for women during menopause. Still, diagnosis can be challenging, treatments need to be multidisciplinary and improvement can be slow. In fact, up to 80 per cent of people go undiagnosed even after one or more fractures, according to a federal action plan for osteoporosis. “It often falls off the radar,” says Professor Markus Seibel, an endocrinologist at the University of Sydney. “Osteoporosis is just not always recognised for what it is – a very frequent disease that’s often progressive.” Even so, bone loss and fractures are treatable and preventable.
So how does bone get lost and remade? How does osteoporosis get diagnosed? And how can people with low bone density manage and prevent osteoporosis?
![‘Not knowing [what I had] was really, really bad.’](https://static.ffx.io/images/%24zoom_0.369%2C%24multiply_0.7725%2C%24ratio_1.5%2C%24width_756%2C%24x_0%2C%24y_0/t_crop_custom/q_86%2Cf_auto/4841c1e291843acb467d564abd28fc869ab0848f)
Elaine Cotter: ‘Not knowing [what I had] was really, really bad.’Credit: Penny Stephens
What is osteoporosis?
Our skeletons – often portrayed as a symbol of death – are, in fact, very much living tissue during life, made of collagen and minerals such as calcium and phosphate, and filled with cells. All 206 bones of an average adult skeleton, from the femur (our biggest bone equal to a quarter of our height) to the rice-grain sized stapes in the middle ear, go through a process of constant yet gradual renovation called “remodelling”. This means if an adult skeleton was compared with a decade or so earlier, it would be structurally the same but made of different bone.
Across our entire skeleton we have about three million bone remodelling units – a clean-up crew of sorts that includes the cells called osteoclasts, which remove older or damaged bone, and osteoblasts, which form new bone using resources such as calcium, phosphate and proteins from the bloodstream. A third cell, called an osteocyte, is a kind of conductor of the crew, regulating the other cells in response to stimulus such as exercise.
Most people reach peak bone mass in their late 20s or early 30s. “When you’re in your prime, your bone metabolism, your bone turnover, is beautifully balanced,” says Seibel, who has been a clinician-researcher of musculoskeletal diseases for nearly 40 years. “And then age, menopause, diseases such as chronic inflammation or malnutrition – hits as we get older and this finely tuned balance gets out of whack.”
Osteoporosis, from the Greek “porous bones”, deteriorates the microscopic structure of bone – eventually enabling seemingly innocuous trauma to possibly fracture the bone. “I’ve seen people get a broken spinal bone by just turning around to pick up a cup of tea,” says Professor Peter Ebeling, who leads the department of medicine at Monash Health. How does bone become this fragile? It comes back to osteoclasts being more powerful cells than osteoblasts and the disease causing an imbalance between them. When the two cells do not act in balance – either because osteoblasts stop performing, or both cells work too hard or too little – the osteoclasts dominate and reabsorb too much bone.
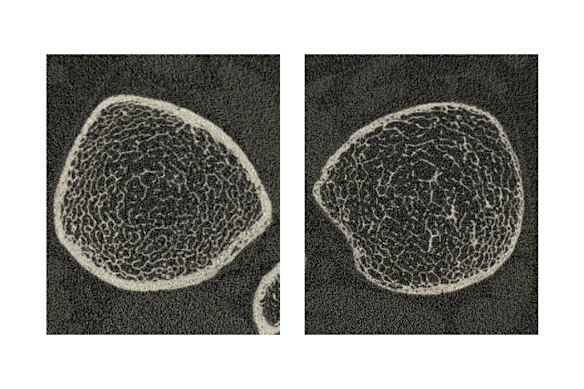
Left, a scan of the trabecular bone of a healthy tibia. Right, a tibia with osteoporosis.
Osteoporosis takes hold both on the solid, outer layer of bone (the cortex) and the inner trabecular bone – a honeycomb-like structure that reinforces the strength of the bone. In fact, the more trabecular a bone has, the more risk there is for osteoporosis causing damage – bones with more trabecular such as the spine and hip are more vulnerable to fracture.
If undetected and untreated, osteoporosis can lead to multiple fractures. A fracture in the spine, for example, might shift load enough that a second vertebrae fractures. Or someone might become inactive from the first fracture, which weakens muscles and increases their risk of having a further fracture. “I’ve had patients who by the time I saw them had four or five osteoporotic fractures,” says Seibel. “We call this the domino effect. So it’s like one fracture ticks over to the next one and the next one.”
Osteoporotic fractures of the spine often lead to kyphosis, where the spine curves forward, creating a stooped posture. In severe cases, this can affect breathing and cause heart problems. Elaine says she has lost about seven centimetres of height as a result of kyphosis. “I do get tired at the end of the day. I find that when I don’t decompress – which means lying flat on the bed for about 10 or 15 minutes throughout the day – towards the evening, I’m really stooped forward. I just feel like I can’t straighten up at all.”
Peter Ebeling: ‘I’ve seen people get a broken spinal bone by just turning around to pick up a cup of tea.’
What can cause osteoporosis?
Overall, the condition is a complex interplay between bone cells on the one side, and hormones and organs on the other. However, exactly what causes osteoporosis will vary from person to person. “There’s many, many factors that lead to bone loss,” says Seibel. “We were never meant to live to the age of 50 or 60. Until not long ago, the average life expectancy was 30 to 40 years ... But then modern medicine came in, and now we live to an age of 80 or 90. So with that kind of longevity obviously comes problems.”
One in three women and one in five men over the age of 50 worldwide have osteoporosis. Menopause is a primary reason for the difference. Estrogen – a hormone that regulates the sexual and reproductive development of females – normally slows bone resorption by inhibiting osteoclasts to maintain bone strength during reproductive years. The reverse occurs when estrogen levels fall. The average age of menopause is 51, although it generally happens at any age from 45 to 55. Even so, bone loss begins during perimenopause when menstrual cycles haven’t stopped but are becoming irregular and hormone shifts are fluctuating.
‘We often describe women after menopause as either ‘fast losers’ or ‘slow losers’ of bone.’
In hindsight for Elaine Cotter, menopause seems like an obvious starting point for her aches and pains. “I felt the usual things with menopause, the hot flushes and things like that.” Even though she works as a practice manager in a GP clinic, she says, “it was never in the front of my mind. I’m staggered that I didn’t think of it myself earlier.”
Loss of bone density due to menopause can affect women at different rates, says Jasna Aleksova, a metabolic bone specialist at Monash Health and St Vincent’s. “We often describe women after menopause as either ‘fast losers’ or ‘slow losers’ of bone. For some, bone loss occurs at around 1 per cent and only for about five years, leading to a relatively modest 5 per cent loss. Others may lose closer to 2 per cent per year, and if this continues for up to a decade, that can be up to around 20 per cent of total bone mass.”
Some of the main risk factors affecting the severity of osteoporosis are genetics, nutrition and lifestyle. Men, who share these risks too, are more likely to suffer from osteoporosis after they reach 60. Males also need estrogen, much of it converted from testosterone, to build bone. Age as well as conditions such as hypogonadism – when people don’t produce enough sex hormones – can disrupt this process and lead to osteoporosis.
The body naturally loses a small amount of calcium through urine. However, kidney problems can cause people to excrete too much calcium. Kidney disease can also disrupt the body’s use of vitamin D, which is crucial to absorb calcium from food. And some medications such as cortisone or anti-epileptic drugs can cause rapid bone loss and multiple fractures. When specialists look for a cause, the bottom line, says Seibel, is “you need to look at this in a holistic way – your body, every organ, every cell, is interconnected in some or other way with everything else”.
Markus Seibel: ‘Osteoporosis is just not always recognised for what it is – a very frequent disease that’s often progressive.’
How is osteoporosis diagnosed?
Peter Hall had just turned 50 when his partner gave him a hug one morning before work. He felt a pain in his back and stomach, and he thought it might be reflux. His GP sent him for tests for a stomach infection, which came back positive. But the pain didn’t go away after treatment. He returned to the doctor who noticed Peter’s back was stiff. X-rays showed five fractures in his lower spine. He then went to get a bone mineral density scan, which showed he had severe osteoporosis. “I was a male, reasonably fit and had a good diet, so I didn’t tick all the typical boxes.”
‘You’ve got no idea what’s going on until something snaps.’
The scan, a dual energy X-ray absorptiometry, or DXA scan, measures the calcium content in an area of the bone such as the spine or hip. Doctors then measure the results against the average for young adults of the same sex and ethnic background to arrive at what’s known as a T-score – the average is a score of 0, while above average is a positive number and below average a negative number. According to World Health Organization guidelines, people with a score -1 to -2.4, have low bone density, also known as osteopenia. People with a T-score below -2.5 are classified as having osteoporosis. (Peter’s DXA scan showed he had a T-score of -3.5 in his lumbar spine.) The scan is covered by Medicare for people 70 or older, and for people already diagnosed with an osteoporotic fracture, or with conditions that put them at risk of it such as kidney disease or therapy with cortisone. Others have to pay out of pocket, which can be between $80 and $120.
Loading
However, the results don’t tell the whole story. Markus Seibel takes issue with the scan being used as the only tool for diagnosing osteoporosis. “Bone mineral density is important in the diagnostic process, but it is only one piece of the puzzle, and it’s critical to understand how to interpret the results within the clinical history of the patient.”
In people who have had a fracture, a key indicator of osteoporosis is whether it happened with “minimal trauma”. As Jasna Aleksova puts it: “Any major trauma, like a car accident, can potentially cause a fracture – even concrete can break. But when a fracture occurs after a minor incident, such as a simple fall from standing height, that is an indicator of osteoporosis.” Seibel says a common trap is for a health practitioner to see a patient with a fracture and disregard osteoporosis if their T-score is better than -2.5. “The important thing to know is that numerically, for most women – we don’t have good data for men – but most women fracture in the so-called osteopenic range.” (The osteopenic range is between -1 and -2.4.)
One problem is the disease silently creeps up on people until there’s pain from a fracture. Says Hall: “You don’t know about it, you’ve got no idea what’s going on until something snaps.” This is unlike osteoarthritis, for example, where degraded joints come with aches, stiffness and swelling. People (and their doctors) can try to screen for risk factors that could lead to osteoporosis: someone might have a family history of hip fractures, or a woman who’s going through menopause might get a precautionary scan. In patients who have significant risk factors for bone loss but no fracture, Seibel will weigh this with the results of the DXA scan. “If that bone mineral density is significantly low, then I can say, ‘All right, you haven’t had a fracture yet, but your risk of having a fracture in the future is [still] quite high.’”
Peter Wong: ‘We know that if you have a hip fracture, you have a really high chance of breaking another bone.’Credit: Courtesy Health Bones Australia
How is osteoporosis treated?
Peter Wong, a rheumatologist and medical director of Healthy Bones Australia, becomes dismayed when he sees patients who have had multiple fractures in the past without being treated for osteoporosis. “No one thinks, goodness, could we do something to prevent it? And we can because we know that the medications we give reduce your chance of breaking a bone, they don’t eliminate it, but reduce your chance by between 30 and 50 per cent. That’s a good offer.”
Indeed, some patients can fall between the cracks, says Peter Ebeling. “At the moment, patients come into hospital with a broken bone, they’re treated by the orthopaedic surgeon, and the fracture is fixed up, but the orthopaedic surgeon isn’t interested in the underlying cause of the fracture because they’re busy treating all these fractures.” In NSW, one solution has been to refer all fracture patients to a fracture liaison service, where doctors assess them for osteoporosis and start treatment. Ebeling has found the program does save the health system money in the long term but, “it’s a preventative strategy, and it hasn’t really been taken up in the other states”. (In 2019, the federal strategic action plan for osteoporosis stated one of its aims was to roll out the service “across the majority of hospitals in Australia”.)
The common medications doctors prescribe are called antiresorptive drugs, which inhibit osteoclast activity and thereby bone loss. “They don’t actually create new bone but they make the bone stronger, so that’s why the bone density improves,” says Ebeling. These can involve oral medications, intravenous infusions or injections.
The most common injection, called Prolia, is given at six monthly intervals. However, says Seibel, there are risks with the drug if people go off it without a replacement treatment such as an oral bisphosphonate because stopping Prolia causes osteoclasts to go into overdrive, which leads to bone loss. Reasons for people going off it can be rare side-effects, or if the patient doesn’t attend their appointment for the next injection. “I have seen people lose 20 per cent of bone in one year, and that’s a lot, after going off Prolia without subsequent therapy,” says Seibel. These problems don’t occur with other anti-resorptive drugs, he notes.
Loading
For patients with more severe osteoporosis, there’s another class of drugs that stimulate cells that create new bone called anabolic treatments. The main drug is called teriparatide, which doctors tend to prescribe for 18 months before switching the patient to an antiresorptive drug to maintain and consolidate the newly formed bone. There is also romosozumab (sold as Evenity), a monthly injection for one year that both increases bone formation and decreases bone resorption. It is one of the strongest drugs for treating osteoporosis – a large clinical trial showed it lowered fracture risk by 73 per cent – but comes with risks for people already vulnerable to heart attack and stroke.
Surgery can follow fractures to fix the bone and prevent further weakening from the person being immobile. “Almost everyone with a hip fracture needs an orthopedic surgeon to fix the acute fracture so they can start walking again,” says Peter Wong. “But we know that if you have a hip fracture, you have a really high chance of breaking another bone in the next 12 months. And so everyone with a hip fracture should be put on treatment for osteoporosis.” Surgery can be difficult given the fragility of the bones (Wong recently had a patient who needed screws put into a vertebra and the surgeon remarked “it was like putting nails into tofu”.)
![‘The sorts of impact [training] you need to do has to really jolt you.’](https://static.ffx.io/images/%24zoom_0.369%2C%24multiply_0.7725%2C%24ratio_1.5%2C%24width_756%2C%24x_0%2C%24y_0/t_crop_custom/q_86%2Cf_auto/8882b214b32323cd052f7e9750ede0b29b8efe61)
Belinda Beck: ‘The sorts of impact [training] you need to do has to really jolt you.’
How can exercise and diet make a difference?
Elaine Cotter avoided exercise for most of a decade after she first felt back pain. “I’m deconditioned to the max, I would say,” she tells us. In the past few months the 61-year-old started a research trial for people with osteoporosis. In the past, muscle strengthening exercises not tailored to her condition would leave her in pain. “I had fractures that weren’t healing because I kept on aggravating them.”
Belinda Beck, a professor at Griffith University and director of The Bone Clinic, started the clinic in Queensland to specifically treat osteoporosis. “People used to think you have to do very gentle exercise so that you don’t increase your risk of fracturing; do things like swimming and walking and yoga and Pilates. But we just discovered that sort of exercise is completely useless for bone in terms of building it.”
Beck, one of the few researchers to lead randomised controlled trials into exercise and osteoporosis, has found that for older people with osteoporosis, high intensity resistance training increases their bone mineral density. Across several studies, Beck has also found exercise more than halved the incidence of fracture. “This is heavy lifting and impact. It’s everything that the doctors think is too scary for people with osteoporosis, but the trick is just supervision,” she says.
Under load from weights, bones bend subtly and osteocytes (the conductor cells) remove an inhibitor on bone formation. “If the load is high enough that [the bone] could break,” Beck says, “it makes the bone cells produce more bone, which builds it up ... to stop it happening to the extent that it might fracture.”
Loading
For there to be results, weights need to be heavy and there needs to be some impact, which she says is “anything that jolts the body when landing on the feet”. “So the impact is not just walking. We’re all used to walking. Even running, it seems like when we’re running it’s a high-impact activity, but it’s not because we bend our joints to absorb the shock. Actually, the sorts of impact you need to do has to really jolt you.” Her program involves only free weights to help people improve their sense of balance, too.
Elaine’s exercises, which she has learned through a different research trial, involve balance training such as walking with one toe in front of the other, and strength training: lifting dumbbells, sitting and standing repeatedly from a chair, and using a box to step up and down. “Some things I couldn’t do. When you go on all fours, hands and knees on the ground – I couldn’t do that because I couldn’t get up,” she says. “But it’s tailored to each participant.”

Elaine Cotter: ‘I’m now doing a kind of exercise that doesn’t leave me bedridden for a couple of days.’Credit: Penny Stephens
Exercise, together with diet, also helps regulate body weight, which in turn influences bone health. Being underweight is particularly problematic because muscle exerts force on bone to stimulate its formation, says Jasna Aleksova. “When you are underweight, you lack the muscle mass and the adipose tissue needed to support optimal bone remodelling.”
‘There’s always that fear that what if I fall? What if I have a car accident? What’s going to happen?’
As for diet, this should include about one gram of calcium a day, which is generally three servings of calcium containing foods such as a tub of yoghurt, slices of cheese, nuts such as almonds, or a 250-millilitre cup of milk. (Elaine eats cheese and yoghurt and drinks almond milk most days to reach her calcium requirements.) About 30 per cent of Australians have a vitamin D deficiency, a hormone that is needed to absorb calcium from the gut to put it into bone. Vitamin D levels can be increased through adequate sun exposure, dietary supplements or some foods such as fatty fish and eggs. Sufficient protein intake is just as important too as it helps the body make the building blocks of bone such as collagen.
Health practitioners will usually monitor results with yearly scans, although they can start to see the difference from medication, exercise and dietary training within six months. When Elaine first had her bone density scan six years ago, the average in her spine was -4.5. Today it’s -2.9. “I feel that I’ve improved, results wise. But there’s always the risk of fracture,” she says. “There’s always that fear that what if I fall? What if I have a car accident? What’s going to happen? … It’s like your life stops for a while until you heal.”
She sometimes asks herself what she could have done differently. “I don’t know whether I could have stopped it from happening. But I know it probably would have been so much different if I knew this is the time I need to start looking at bone health.” She worries when she hears people say their bones aren’t something they need to start thinking about until old age. “I feel I was robbed of my middle age. I went from young to old straightaway.”
This Explainer was brought to you by The Age and The Sydney Morning Herald Explainer team: editor Felicity Lewis and reporters Jackson Graham and Angus Holland. For fascinating insights into the world’s most perplexing topics, sign up for our weekly Explainer newsletter. And read more of our Explainers here.

Felicity Lewis, Jackson Graham and Angus Holland.Credit: Simon Schluter